
Developing a strategy for airway managemenT
The process of airway planning can be considered according to the following components:
Assessment: of patient, situational and clinician factors that might contribute to airway management becoming challenging in a given context.
Anticipation: of challenges that might arise as a result of the above factors.
Consideration: of the most appropriate strategy to address these challenges.
Communication: of primary plan and successive contingencies (including optimisations and triggers for progression) to the team.
Organisation: of resources to maximise the chances of success with the chosen strategy. This includes selection of the most appropriate environment for airway management, ensuring availability of the required equipment and that the necessary personnel are both available and briefed.
The authors of the 4th National Audit Project (NAP 4) in the UK stressed that the end result of the planning process should be an implementable airway strategy. The Vortex Approach defines an airway strategy as “a coordinated series of implementable plans, each a contingency for the failure of the previous one, including clear triggers & defined actions that outline the process of priming for CICO rescue”. A strategy thus not only outlines the initial plan for airway management but is also repeatedly able to answer the question "What is the plan if that plan fails?". Effective planning takes a team whose training and experience has made them competent to manage an airway emergency and ensures that they are capable (via timely access to appropriate resources) and ready to manage it in a specific context.
The Vortex Approach provides a number of resources to assist with airway planning that utilise the same concepts and language as the primary Vortex tool. By using a consistent template for both the planning and implementation phases of airway management the Vortex Approach aims to facilitate recall of the airway strategy and optimise team performance under pressure.
AIRWAY ASSESSMENT: 'evaluating risk' versus 'predicting difficulty'
It must be recognised that the purpose of airway assessment is to evaluate the risk of encountering challenges during airway management rather than to definitively predict whether or not a challenging airway will be encountered. This distinction, and the language used to describe the conclusions reached during airway assessment, may have important psychological consequences that impact on a clinician's willingness to escalate the level of preparedness for a challenging airway.
The commonly used phrases "predicted difficult airway" or "anticipated difficult airway" imply that a determination has been made that airway management will actually present a challenge - with the corollary that the conclusions of the airway assessment were incorrect if airway management subsequently proves to be uneventful. Being perceived to have been 'wrong' may lead the both the airway operator and their team to infer that any escalations in preparedness to deal with airway challenges were inappropriate and that their implementation represented an overreaction. This attitude can represent a significant psychological barrier to preparing appropriately for future events.
In contrast, the concept of identifying an "increased risk" of a challenging airway provides for the contingency that its likelihood may be significant, without being certain - or necessarily even probable. Given the lack of specificity/sensitivity of many of the known risk factors for a challenging airway, it is reasonable that the perceived risk may be sufficiently elevated to warrant escalating preparedness (or conversely that failure to escalate might be viewed as complacent) while still acknowledging that it remains more likely that a normal airway, rather than one which is challenging, will be encountered.
“the determination of whether the conclusions reached from the airway assessment, and the airway strategy subsequently adopted, were warranted should be based upon appropriately identifying the risk of a challenging airway, not whether those challenges actually manifested - in other words you don’t need to be to be right, you need to be justified.”
As such, the determination of whether the conclusions reached from the airway assessment, and the airway strategy subsequently adopted, were warranted should be based upon appropriately identifying the risk of a challenging airway, not whether those challenges actually manifested during airway management - in other words you don’t need to be right, you need to be justified. It is logical that airway assessment can correctly identify an increased risk of a challenging airway, warranting an escalation in preparedness to address this, yet airway management proves to be uneventful. In such a situation the concept of "predicted difficult airway" tends to reinforce the idea that the conclusions reached from airway assessment were wrong because they failed to correctly predict the outcome. Conversely the concept of "elevated risk of a challenging airway" favours the risk assessment being viewed as correct, despite a normal airway being encountered. This helps to overcome hindsight bias based on previous encounters and gives clinicians permission to prepare appropriately for airway management. Moreover, as is discussed below, rather than make a general assessment of whether there is an increased risk of a challenging airway, a specific assessment should be made of whether there is a increased risk of facing challenges with each of face mask, supraglottic airway, endotracheal tube and CICO Rescue. This facilitates development of an appropriate airway strategy.
In addition to the above considerations related to risk perception, it should also be noted that simple interventions such as meticulous attention to positioning, etc in response to an assessment of increased risk, may in fact be responsible for subsequent airway management being uneventful and further progression of the airway strategy being unnecessary.
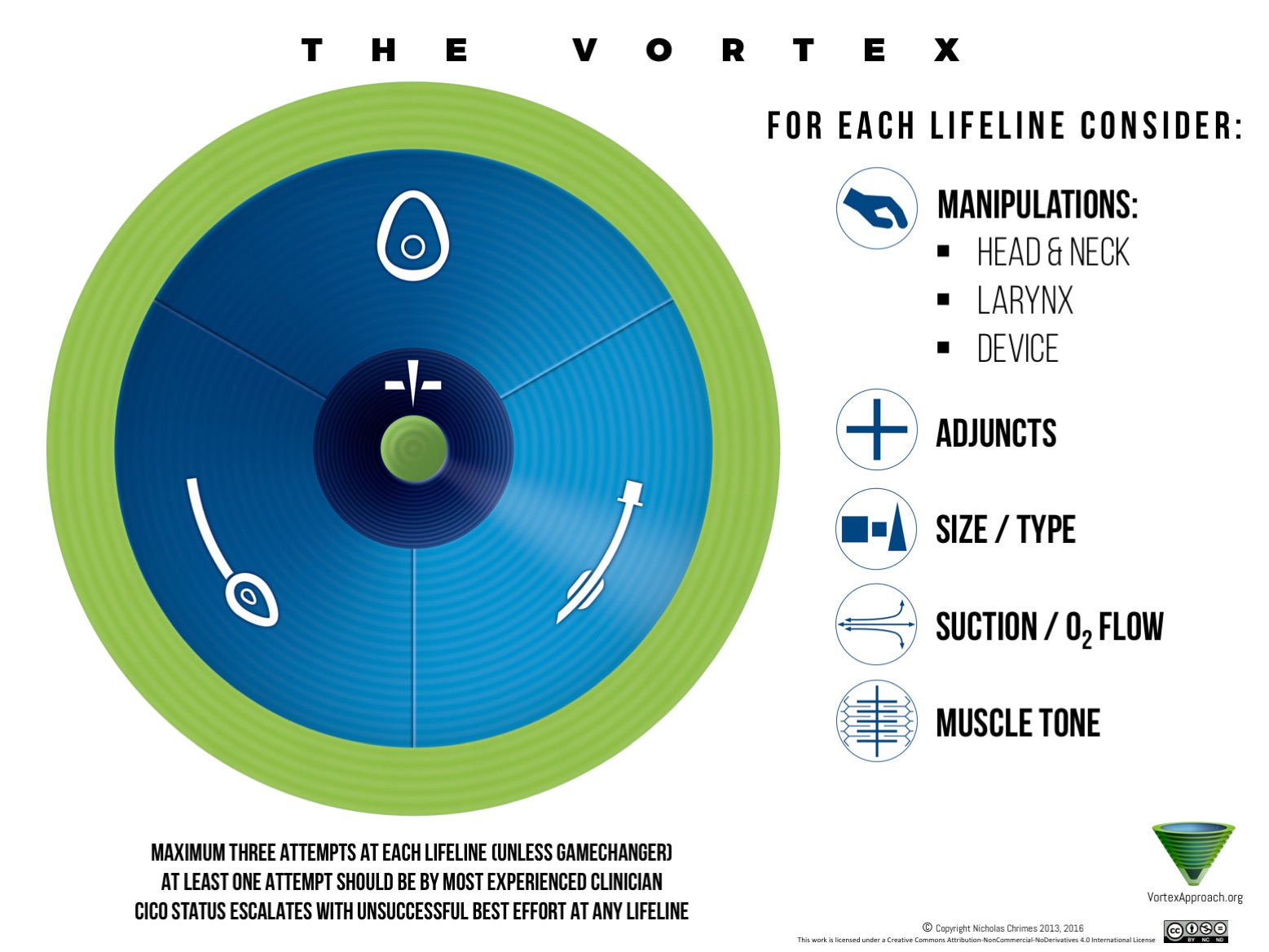
The Vortex Airway Assessment Tool
The Vortex airway assessment tool is designed to be used in real time during the preparatory stages of airway management. It prompts clinicians to consider broad categories of factors that can contribute to the risk of airway management becoming challenging in order to reduce the likelihood that key considerations are overlooked. Rather than restricting these prompts to the anatomical features of the patient, the Vortex assessment tool also acknowledges situational and clinician factors that can compound the impact of challenging airway anatomy as well as consideration of the predicted safe apnoea time available for any identified challenges to be overcome. The objective is to encourage a more holistic evaluation of the likelihood of the patient being exposed to sustained hypoxia during airway management in a given context.
Airway assessment should not be restricted to considering factors which might make intubation challenging. The likelihood of encountering challenges to establishing alveolar oxygen delivery via all three of the upper airway lifelines as well as CICO Rescue should be assessed according to the prompts on the tool.
In addition to considering these factors prior to the initiation of airway management, the factors listed on the airway assessment tool should also be considered prior to withdrawal of airway support as many airway emergencies occur during the process of the patient resuming maintenance of their own airway during emergence (e.g. following extubation).
Australian & New Zealand College of Anaesthetists Airway Assessment Document
The specific indices that should be assessed under each of the headings listed on the tool and their implications for evaluating the risk of a challenging airway is an important part of clinician training that is beyond the scope of the Vortex Approach. Other airway resources should be consulted for this purpose. An example of such a resource, provided by the Australian & New Zealand College of Anaesthetists, is available by clicking on the link on the left.
The following overview is provided simply to provide examples of the types of factors intended to be prompted by each of the listed headings. It is not intended to be an exhaustive list of the factors intended to be prompted under each category.
PATIENT FACTORS:
Airway History: previous challenges with face mask ventilation, supraglottic airway, endotracheal intubation or CICO Rescue according to patient or medical record. This should include consideration of any difficulties encountered during initiation of airway management prior to withdrawing airway supports, as this may influence what constitutes an appropriate withdrawal strategy.
Predisposing Conditions: conditions known to be associated with an increased risk of a challenges with one or more of face mask ventilation, supraglottic airway or endotracheal intubation. These include but are not limited to certain congenital syndromes, pregnancy, obstructive sleep apnoea, risk of massive regurgitation, poor patient cooperation, epiglottitis, anaphylaxis, etc.
Appearance: the overall appearance of the patient may provide valuable clues about the risk of challenges arising during attempts to establish alveolar oxygen delivery via the lifelines &/or CICO rescue. This may include more obvious signs such as a large beard or receding chin as well as more subtle combinations of factors which may not necessarily individually meet the usual criteria for identifying the difficult airway. This latter 'gestalt approach' to airway assessment is an important method by which experienced airway clinicians might be able to identify some potentially challenging airways that are not flagged by the standard metrics.
Distortion: presence of masses or other causes of airway asymmetry including haematoma or infection
Trauma: this may be acute physical/chemical trauma or evidence of previous trauma from accidents, surgery or radiotherapy. The potential for trauma and deterioration of the airway while a patient is intubated (e.g. during airway or cervical spinal surgery) should also be considered as it may lead to the occurrence of a difficult airway at extubation.
Obesity: may impact on ability to achieve entry into the Green Zone via the lifelines or CICO Rescue. Distribution of body fat is also an important consideration.
Mouth: standard assessments including mouth opening, mallampatti score, teeth, ability to prothagnate, oropharyngeal pathology, etc.
Neck: thyromental distance, neck extension, need for manual in-line stabilisation, neck circumference, etc. Where potential distortion of laryngeal anatomy may impact on the ability of structures to be easily recognised, evaluation of the internal structures of the neck via nasendoscopy should be considered.
Safe Apnoea Time: the assessment of the likelihood for potential challenges with airway management must be done in the context of how much time is likely to be available before the patient critically desaturates. Factors which decrease the functional residual capacity, impair gas exchange, increase oxygen consumption, decrease oxygen delivery to the tissues (anaemia, low cardiac output) or impede the ability to effectively preoxygenate/apnoeically oxygenate the patient will impact on the time available for any identified challenges to be overcome and thus the degree of hypoxia to which the patient will be exposed. Considering the safe apnoea time provides a context which should influence the threshold for instituting additional precautions for a identified risk of encountering a challenging airway. In addition precipitous desaturation will increase the psychological stress to which the airway operator is exposed, potentially impairing decision making and motor skills and thereby magnifying any challenges presented by the anatomical, situational or clinician factors.
SITUATION FACTORS:
Emergency: the context of an emergency often involves a constellation of other factors that can make airway management more challenging. These include stress, time pressure, need for cricoid pressure, the distractions of an unwell/unstable/uncooperative patient, etc.
Location: retrieval settings, emergency departments, intensive care units, wards or 'off the floor' anaesthetic locations can all potentially increase the degree of challenge posed by managing a given airway. Even within an operating room environment there may be a variation in the ease by which a challenging airway can be managed between different institutions. Factors including staff, equipment, lighting etc. may all contribute to variations in the challenges faced in these environments and assessing their impact will depend on clinician understanding of the specific environments involved. In addition to the physical location, "temporal location" should also be considered, as the resources available and ability to manage challenges effectively in any one location may vary substantially according to the time of day. The ability to alter both physical and temporal location for initiating airway management should always be considered as part of airway planning.
CLINICIAN FACTORS:
Experience: inexperience of the airway operator and their team will augment the degree of challenge presented by any given set of factors and should lower the threshold for instituting additional precautionary measures (including seeking senior assistance).
Fatigue/Stress: clinician fatigue or stress may impact on a clinical team's cognitive, motor & communication skills, impairing their ability to effectively manage a challenging airway.
developing aN airway strategy using the Vortex Approach
Developing an airway strategy involves addressing each of the domains of the Vortex tool: Lifelines, CICO rescue & Green Zone
Following assessment of the patient, situation & clinician factors impacting on airway management, developing any airway strategy requires addressing each of the domains of the primary Vortex Tool: the Green Zone, the upper airway lifelines & CICO Rescue.
1. Green Zone: with the exception of acute airway obstruction or extreme hypoxia (in which there will be no opportunity to develop a strategy anyway), airway management begins in the Green Zone - as even in situations in which the airway is already partially compromised or the oxygen saturations are low, adequate alveolar oxygen delivery is occurring. While still in the Green Zone, the options for initiating management of the airway, as well as the most appropriate course of action if the Green Zone is re-entered during the process of airway management (by a lifeline other than that desired), should be considered. Use of the Green Zone tool for this purpose is discussed in more detail below.
2. Lifelines: the sequence in which each of the lifelines of face mask, supraglottic airway & endotracheal tube are to be attempted and the optimisations to be implemented for each should be anticipated. As many optimisations as possible for each lifeline should be implemented prior to initiating airway management. This enables the first attempt to be as close as possible to a 'best effort' and ensures that remaining optimisations to achieve a best effort are identified in advance and able to be implemented efficiently if needed. The Vortex tool can be used to prompt potential optimisations for each of the upper airway lifelines.
{kind=link}
3. CICO Rescue: the need for priming for CICO rescue should be considered and if necessary initiated using the CICO Status tool.
Once a strategy has been developed using the Green Zone, Vortex & CICO Status tools, confirmation of readiness to initiate airway management - including ensuring availability of appropriate drugs/equipment/monitoring and role allocation to team members - can be coordinated using the Vortex Airway Strategy Tool.
{kind=link}
The Vortex Airway strategy tool
Designed to be used by any discipline, in any context requiring planned airway management, this tool provides a “pre-flight checklist” which prompts confirmation of key aspects of safe airway management prior to induction and specifically reinforces the Vortex Approach template during the preparation phase.
The aim is that by reinforcing the Vortex Approach format during routine preparation, this will facilitate its implementation when a challenging airway is encountered. It is also hoped that provision of a common checklist for use across different critical care specialities will facilitate development of a shared mental model for airway preparation and improve teamwork in situations when these groups come together.
The strategy tool should be used in combination with the primary Vortex tool the CICO Status tool and the Green Zone decision tool.
Using the Green Zone Tool To develop an airway strategy
When developing an airway strategy the Green Zone tool can be used to plan the initiation of airway management as well as for anticipating options if the Green Zone is entered during the process of airway management.
The same opportunities exist in the Green Zone to optimise physiology, strategise interventions and mobilise resources before initiating advanced airway management, as arise during airway management. The scope of options appropriate for exploring each of these opportunities in a manner which is practical/safe, however, may vary according to context - with a greater array of options typically being available prior to initiation of airway management.
1. OPTIMISE: as with entering the Green Zone during airway management, the opportunity to optimise physiology prior to airway management should prompt consideration of techniques to maximise oxygen saturations & extend the safe apnoea time in case a prolonged interruption to alveolar oxygen inadvertently occurs.
2. STRATEGISE: The options for developing a strategy can still be categorised in the same manner when in the Green Zone prior to initiating airway management, as was described for when the Green Zone has been entered during the process of airway management.
Maintain: when in the Green Zone pre-induction the option of maintaining the airway by which alveolar oxygen delivery is currently being achieved (i.e. the patient maintaining their own airway) includes the potential to perform surgery under regional anaesthesia or to defer a procedure to a later time where feasible.
Convert: converting the patient's airway to a more advanced airway without intending to leave the Green Zone when initiating airway management, includes awake upper airway options such as awake fibreoptic intubation or awake direct/videolaryngoscopy and awake non-emergent front-of-neck options such as awake tracheostomy/cricothyroidotomy. It also includes asleep techniques which aim to preserve continuous ventilation of the patient. In rare situations it may also include the option to transfer the patient to more novel ways of providing blood oxygenation such as initiation of cardiopulmonary bypass before administering anaesthesia. The critical element of the 'convert' option is the intention to maintain the ability to deliver fresh oxygen to the blood (typically may maintaining alveolar oxygen delivery but via artificial means in the rare case of the use of bypass/ECMO) without interruption (remain in the Green Zone) until the alternate airway is established.
Replace: the replace option involves inducing the patient and acknowledging the likelihood of potentially interrupting alveolar oxygen delivery via the occurrence apnoea/obstruction. This represents entering the funnel of the Vortex and is the most common way by which airway management is initiated. When this option is selected to initiate airway management the primary Vortex tool can be used during the planning process to anticipate the sequence in which the lifelines will be attempted and the optimisations likely to be implemented.
{kind=link}
Whatever option is chosen as the initial approach to airway management, the strategy must always include back up plans to address the contingency that the primary and subsequent plans fail and ensure that these are familiar to the team and that the resources to implement them are immediately available. As with developing a strategy when entering the Green Zone during airway management, the team must always be able to answer the question: "What is the plan if that plan fails?". This not only include strategies to optimise attempts at the upper airway lifelines if the Green Zone cannot be re-entered and the patient becomes 'stuck in the Vortex', but also consideration of appropriate ways to exploit the opportunities of the Green Zone if it is re-entered.
3. MOBILISE:
Having developed a strategy the appropriate resources can now be mobilised to implement it effectively.
Personnel: consideration should be given to the need for additional personnel (for consultation, technical expertise or simply as an extra 'pairs of hands'). When exploring this opportunity prior to initiating airway management, it is often possible to source the help of individuals who will take more time to arrive than might be practical to wait after airway management has commenced.
Equipment: the need for specialised equipment to be sourced or prepared (including priming for CICO rescue) should be also be considered.
Location: the appropriateness of continuing airway management in the current location versus moving the patient to a patient more suited to managing particularly challenging airways should be considered. In addition to considering transferring a patient from the ward, intensive care unit or emergency department to the operating suite within a hospital, this option may also involve transferring a non-time critical patient to another specialised institution or, in a pre-hospital setting, evaluating the need to definitively secure the airway prior to transport.