
PLEASE NOTE THAT AIRWAY CARTS CANNOT BE PURCHASED THROUGH THIS SITE. CARTS AND EQUIPMENT MUST BE ORDERED FROM YOUR USUAL SUPPLIERS. GRAPHICS ARE AVAILABLE FOR DOWNLOAD HERE.
The Vortex Implementation Tool
VORTEX AIRWAY RESCUE CART
The Vortex Airway Rescue Cart
The Vortex Airway Rescue Cart differs from most conventional airway carts in 3 important ways:
Dedicated emergency airway cart: the Vortex cart focuses on equipment that is required in the situation when alveolar oxygen delivery cannot be achieved ("in the Vortex"). Equipment required when the patient is in the Green Zone and alveolar oxygen delivery can be achieved (such as that for awake fiberoptic intubation) is able to be sourced from elsewhere. This minimises the amount of equipment stored in the cart, decreasing clutter and improving the ability of clinicians to easily locate the required devices during an airway emergency. Limiting equipment choices also reduces the cognitive load imposed by decision making during an airway emergency as well as providing a training advantage by encouraging clinicians to focus on becoming proficient with a limited number of devices. A limited amount of non-emergency equipment has been retained in the Green Zone drawer - the rationale for this is discussed below.
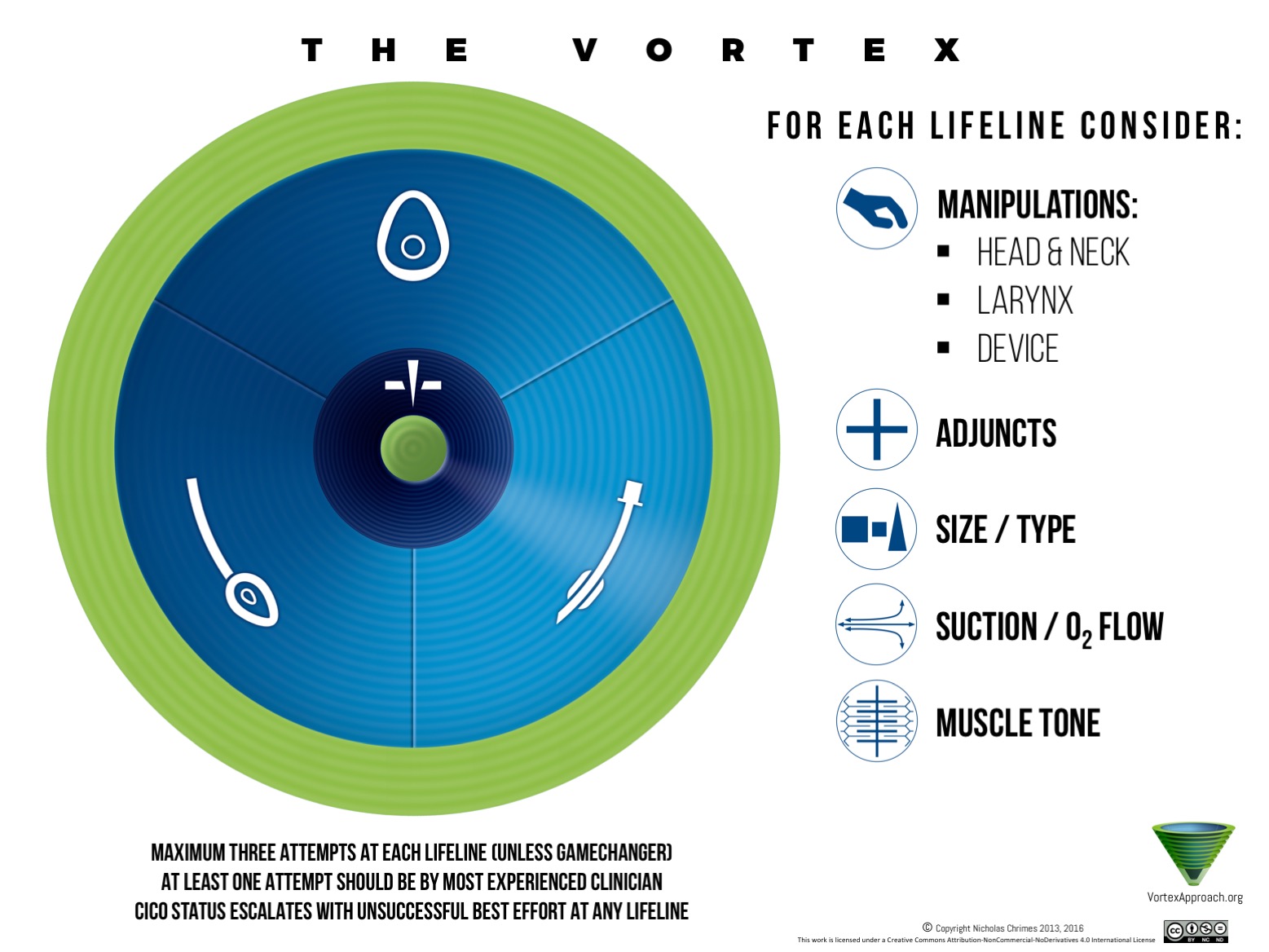
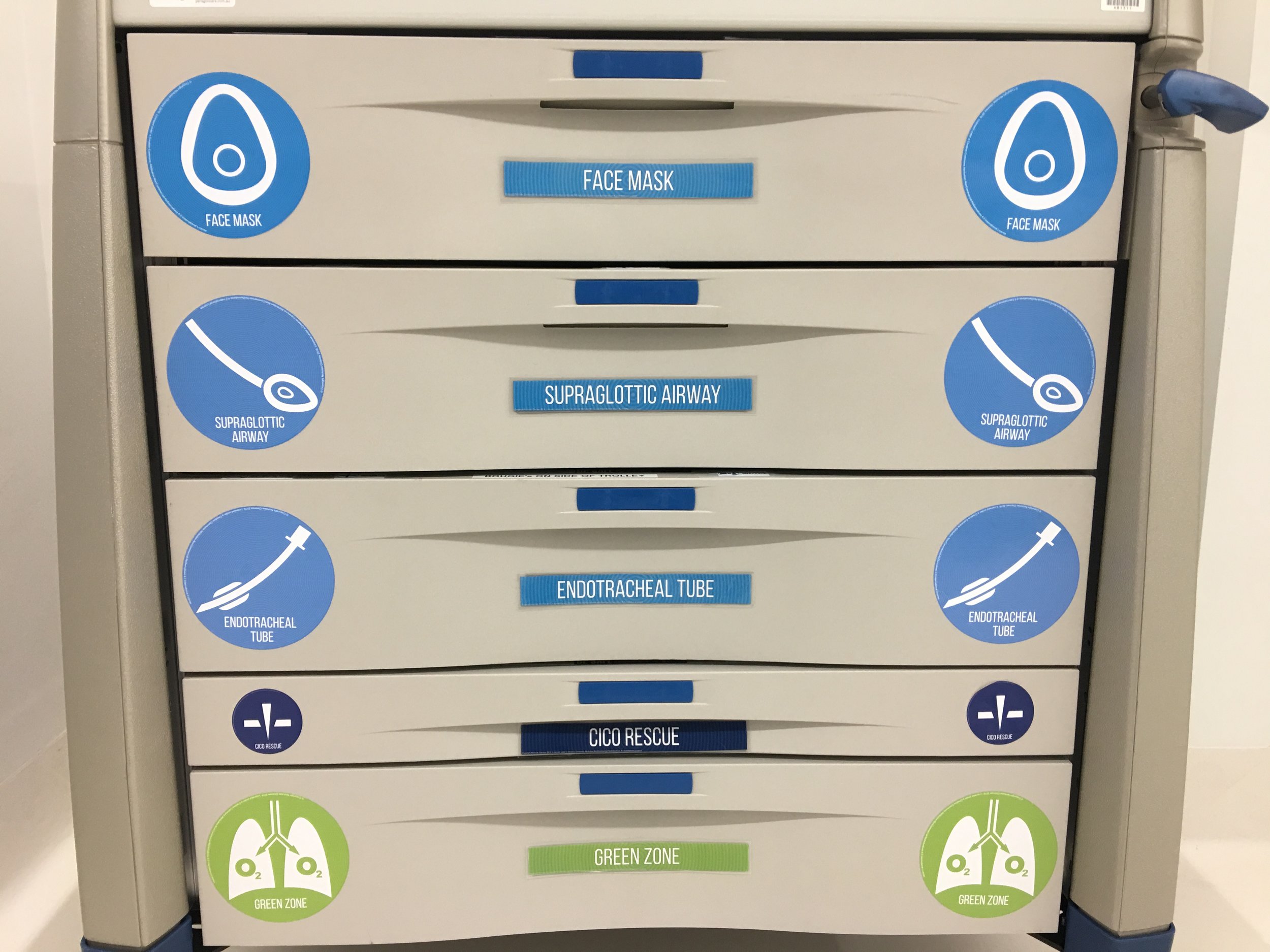
Vortex-based layout and icons: each drawer of the cart corresponds to one of the 5 domains of the circular Vortex graphic. Within the drawers corresponding to each of the upper airway lifelines, equipment is arranged according to the 5 optimisation categories on the Vortex implementation tool. Adherence to the Vortex template not only further facilitates easy location of equipment but also allows the cart to prompt clinicians for potential optimisation interventions. This promotes efficient progression towards a best effort at each of the upper airway lifelines.
Prompts for non-equipment interventions: in addition to prompting for use of equipment to facilitate success at each of the upper airway lifelines, the Vortex Airway Rescue Cart also uses visual cues to prompt for non-equipment interventions towards achieving a best effort. These include manipulations of the head/neck, larynx and device as well as the use of drugs to produce muscle relaxation.
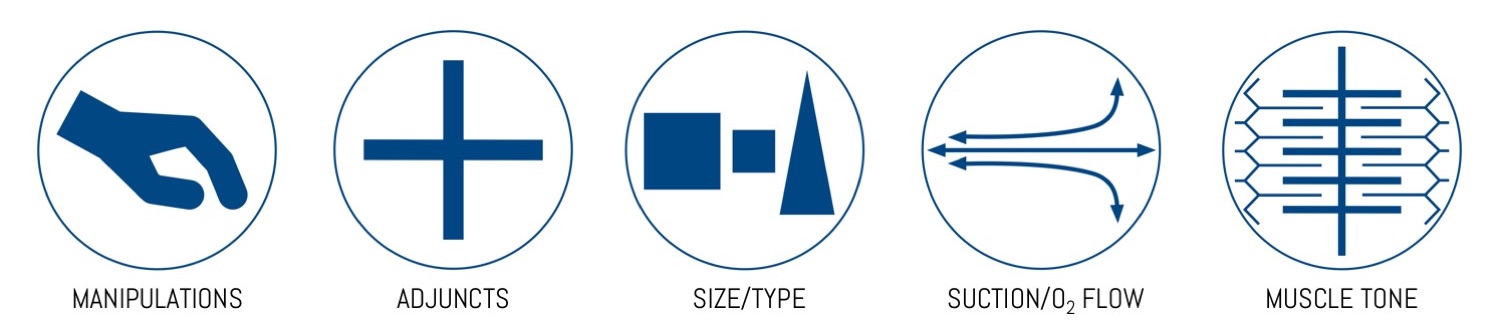
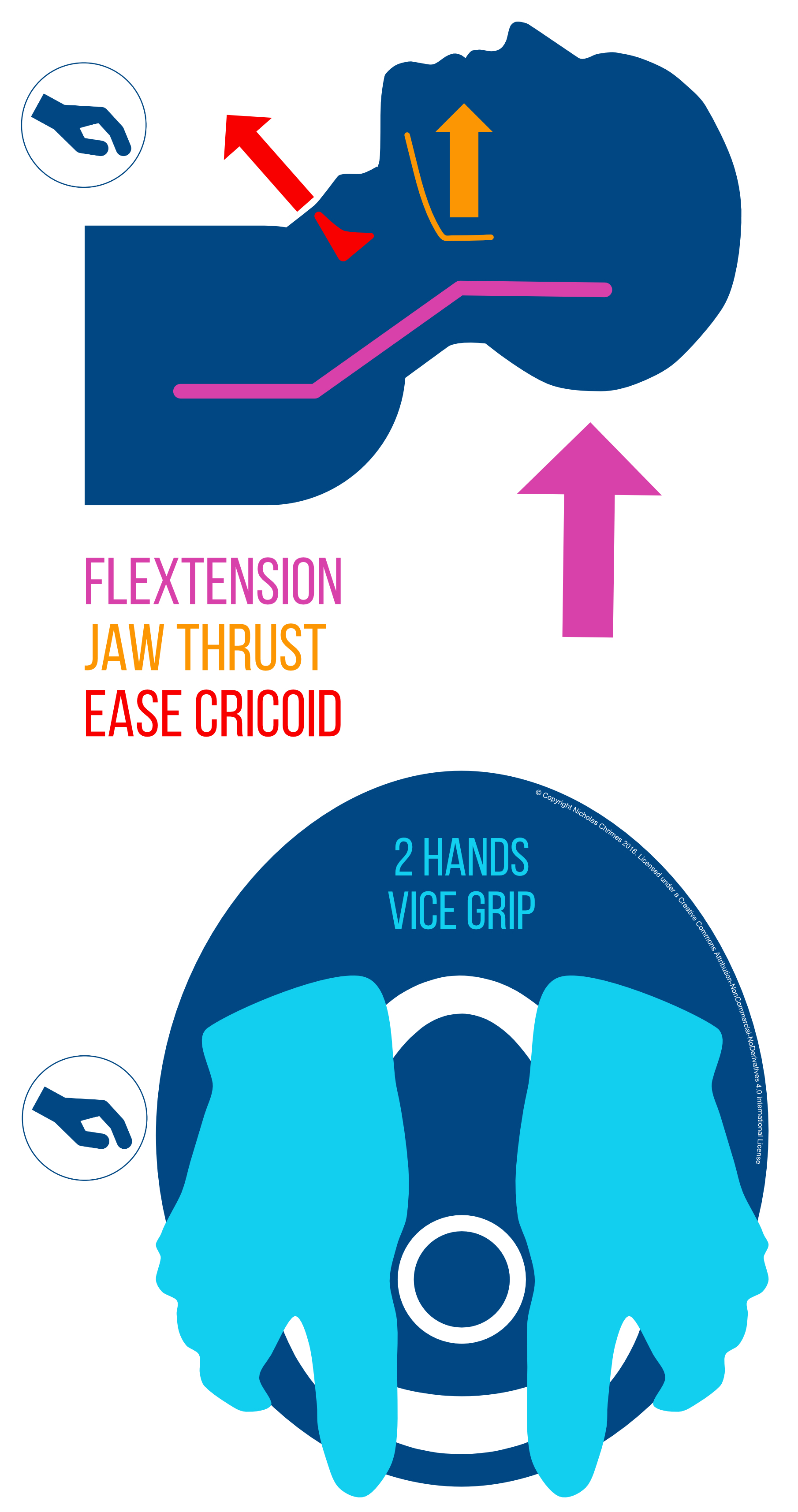
Icons to prompt manipulations of head/neck, larynx and device for FMV
Translation of the categories and icons of the Vortex to the layout of the airway cart is an example of clinical integration of the implementation tool into the working environment. This allows the the airway cart to function as an extension of the implementation tool - both to maximise opportunities to establish an airway using one of the upper airway lifelines and to promote recognition of when optimisation strategies for a given lifeline have been exhausted, providing the clinical team with permission to move on to alternative techniques.
The anticipated benefits to the airway assistant of using a single consistent template for both the implementation tool and airway cart are twofold:
Familiarity with the Vortex tool makes it easier to consider the need for interventions and locate equipment, which facilitates use of the airway cart.
Familiarity with the airway cart reinforces the specific interventions that the optimisation categories for each lifeline refer to, which facilitates use of the implementation tool (in both current and future episodes of airway management).
In addition, the use of a constant template allows other team members, familiar with the Vortex Approach to track the progress of airway management and contribute suggestions in a structured manner. These factors are intended to enhance team performance and potentially improve patient safety during all episodes of airway management. Maximising the benefits provided by use of the Vortex Airway Rescue Cart requires that clinicians are trained in use of both the Vortex Approach and the airway cart.
Ideally carts should be standardised across all sites in an institution where airway management takes place. While variation in the specific contents may be required to address the distinct clinical needs of different areas (e.g. emergency department versus operating theatre versus intensive care unit).
This brief video demonstrates simulated use of the Vortex Airway Rescue Cart, by a team familiar with the Vortex Approach, to facilitate a best effort at face mask ventilation.
CONTENTS of the VORTEX AIRWAY rescue CART
The content list for the Vortex Airway Rescue Cart below represents a 'menu' of options which are not meant to be implemented exhaustively. Specific equipment for a cart should consist of a limited number of devices, selected according to local preferences, requirements and policies. For simplicity, the minimum number of different devices to meet clinical needs should be selected. In evaluating the need to include different types of devices within a category, consider the following approach:
Distinguish between 'preferred' devices (i.e. different clinicians would choose a different device for the same situation) and genuine 'distinct' devices (i.e. the same clinician would choose a different device for different contexts).
Alternative devices within a category should only be included where different devices are legitimately better suited for different contexts/purposes. For each defined context/purpose, choose the single most appropriate device (ideally based on evidence where available).
Alternative devices should not be included where they arise solely from clinician preferences (i.e. "favourites"). While different clinicians may genuinely have a higher rate of success with different devices in the same context, logically this can only stem from differences in technique or familiarity. In this situation, rather than including multiple devices, ideally the reasons for varied success rates with a given device should first be examined and education provided to address these, in an attempt to ensure all clinicians are proficient with the 'best device'.
Unfortunately evidence for a particular device as 'the best' is often lacking and reliance on clinical experience is required. The "million dollar question" can be a useful strategy to help delineate the most appropriate device for a given indication. The following hypothetical question is posed: "if you were on a game show with an anaesthetised patient in front of you and would win a million dollars if you (achieved relevant goal) on the next attempt, which device would you choose?". This analogy is often reveals confounders in making a decision, such as consideration of secondary goals at the expense of maximising the probability of achieving the primary goal. For all drawers except the Green Zone drawer, this primary goal should be rapid restoration of alveolar oxygen delivery - not protection from aspiration or the ability to subsequently intubate the patient (these ancillary goals should of course be considered if they can be achieved without compromising the likelihood of success at the primary goal). Note that while, when appropriately constructed, the 'million dollar question' helps to focus a choice on primary goals, it does not necessarily determine whether the selection made reflects the best device or simply individual clinician preferences.
Ultimately a balance must be struck between minimising clutter and ensuring the 'right tool for the job' is available. Limiting alternative equipment that is based solely on 'favourites' enhances the utility of the trolley whereas limiting alternatives that are intended to be used for distinct indications impedes it.
Additional details on the rationale for inclusion of some devices and their location within the cart are provided below.
Potential Contents for Vortex Airway Rescue Cart (click to enlarge)

Vortex Emergency Airway Cart: potential contents for CICO Rescue & Green Zone drawers.
UPPER AIRWAY LIFELINE DRAWERS:
Equipment included in these drawers should be limited to that required to optimise the chances of success at restoring the patient to the Green Zone as rapidly and reliably as possible. There should then be time to source other equipment (either from the Green Zone drawer or elsewhere) if there is a plan to either 'convert' or 'replace' the airway with which entry to the Green Zone was achieved.
Supraglottic Airway: the role of a bougie and a laryngoscope in placement of a SGA is described in the section of the website on achieving a best effort at supraglottic airway.
Endotracheal Tube: the empirical use of the combination of a hyperangulated videolaryngoscope, steerable tip stylet/bougie and a bullet tipped ETT to facilitate rapid endotracheal intubation in a time critical situation when direct laryngoscopy is impossible is discussed on the website section on achieving a best effort at endotracheal tube. A fiberoptic scope may also be used as a steerable bougie to facilitate ETT delivery and passage in combination with a hyperangulated videolaryngoscope, either without or with (fiberoptic assisted video intubation - FAVI) a use of a screen connected to the fibrescope.
CICO RESCUE DRAWER:
CICO Status Tool: this should be included and placed on top of other equipment so that it can easily be retrieved for reference in the event that escalation of the CICO Status is required.
CICO Rescue Kits: the inclusion of adult/paediatric kits including equipment for cannula &/or scalpel techniques should be determined according to patient population and local practice/preferences for performance of CICO Rescue. More information on the equipment required in CICO Rescue kits is provided on the webpage dealing with this.
GREEN ZONE DRAWER:
A limited amount of equipment for use once the Green Zone has been entered is included in the Green Zone drawer of the cart. While by definition entry into the Green Zone implies that the requirement for this equipment is not imminently time critical, it's inclusion on the Vortex Emergency Airway Cart is based on the following:
While not being required to manage an emergency, some equipment for use in the Green Zone may still be required with some urgency and thus it is advantageous to have it in the cart.
In some contexts, limited staffing, particularly in combination with a tenuous hold on the airway that has provided entry to the Green Zone, may make it undesirable for the airway assistant to leave the airway operator alone while they source additional equipment stored remotely.
The presence of equipment in the Green Zone drawer is able to act as a prompt for key options in the Green Zone.
If particular pieces of equipment which are only appropriate for use when in the Green Zone are requested in circumstances in which the patient is clearly 'stuck in the Vortex', their presence in a drawer labelled specifically for the Green Zone context provides a prompt for the airway assistant to query their appropriateness in this situation which can improve team situational awareness and potentially avoid the use of inappropriate techniques.
Green Zone Tool: this should be included and placed on top of other equipment so that it can easily be retrieved for reference when the Green Zone is entered.
Intubating Supraglottic Airway: this term is used here to refer to dedicated supraglottic airway devices that are used for the specific purpose of providing a conduit for intubation but would not be used in the absence of a need for subsequent intubation (e.g. the Fastrach LMA - Teleflex). These are distinct from supraglottic airway devices that are in general use which additionally allow passage of an endotracheal tube. Where these dedicated intubating devices are included in the cart they should be kept in the Green Zone drawer rather than the supraglottic airway drawer. The rationale for this is that if the airway is obstructed ('stuck in the Vortex') and rescue is being attempted using a supraglottic airway, the device selected should be that which has the greatest probability of rapidly returning the patient to the Green Zone. For most clinicians this is unlikely to be a dedicated intubating SGA (such as the Fastrach LMA) which is typically relatively unfamiliar compared with other 1st and 2nd generation supraglottic airway devices (in other words it is unlikely to pass the 'million dollar test' outlined above). Selecting a device which has a lower likelihood of restoring alveolar oxygen delivery on the basis that, if it does, intubation will subsequently be able to be achieved via that device, represents a fixation error. The focus at this point should be securing entry to the Green Zone, not intubating the patient. In addition, the Aintree catheter allows intubation via many more familiar supraglottic airway devices once the Green Zone has been entered. In the situation where entry into the Green Zone is possible via face mask ventilation then, in appropriately skilled hands the use of a dedicated intubating supraglottic airway may be appropriate.
Fiberoptic Scope: while other than for fibreoptic assisted video intubation (FAVI), use of a fibreoptic scope is not an appropriate technique if alveolar oxygen delivery cannot be achieved ('in the Vortex'), once the Green Zone has been entered via a face mask, supraglottic airway or even CICO Rescue, the opportunity to convert the airway to an endotracheal tube using the fibrescope may arise. The presence of the fibreoptic scope in the Green Zone drawer both acts as a prompt for consideration of this option as well as ensuring it is readily available if required.
Cuffed Cricothyroidotomy Kit: these kits (e.g. the Melker Kit - Cook Medical) are included in the Green Zone drawer (rather than the CICO Rescue drawer) as using them is is too slow for a technique for CICO Rescue when 'stuck in the Vortex'. Where successful CICO rescue using a cannula technique has provided entry to the Green Zone, however, they provide a useful method to convert the tracheal cannula to a cuffed airway device where this is felt to be preferable to using a fiberoptic scope from above.
Apnoeic Oxygenation Kit: if apnoeic oxygenation (ApOx) was not (able to be) employed prior to induction, then once entry into the Green Zone has been achieved following the occurrence of airway difficulty, the opportunity to reconsider the need for ApOx arises. Initiation of ApOx in this situation contributes to extension of the safe apnoea time in the event that the ability to achieve alveolar oxygen delivery is inadvertently lost during subsequent airway management. Inclusion of equipment for both nasal and buccal ApOx is advocated but the buccal technique is often easier to implement in the unconscious patient, as it involves simply hooking the 3.5 RAE ETT into the left corner of the mouth rather than looping the nasal prongs around the patient's ears (which may require lifting of the head and potentially altering the patient's position or otherwise risking compromise of the airway that provided entry to the Green Zone).
LABELS for Vortex AIRWAY RESCUE CART
The full range of labels for the trolley and the visual prompts for non-equipment optimisations are available from the downloads section of the website.